|
Forum for Clinical and Surgical Oral Pathology
Case BBOPF 22-1
Dr. Kurt Summersgill (University of Pittsburgh, USA) is seeking you input for an unusual case. The case will be posted until February 21, 2022. A summary of the responses will ensue shortly after.
History
74 year-old male referred by a periodontist for oral lesions. The problem began 21 years ago in 2000, soon after placement of implants and full max/mand fixed prostheses. First lesion was on the alveolar ridge and was non-specific. In 2001 a biopsy was non-specific, with subepithelial separation and negative DIF. The lesions continued to spread, and in 2016, a biopsy of the upper lip was signed out as verruciform xanthoma. A 2018 biopsy was signed out as papilloma, but at my review (in December, 2021), it looked like a VX (This was my introduction to the case).
Clinical visit
Italian heritage, US citizen. No foreign travel. The lesions are painful and spreading, most recently in the past two years onto the lower vermilion. Spicy is painful. Cleanings of his implants is painful. The only site spared is the dorsal, lateral, and ventral tongue (except for a 4x4 mm thin leukoplakia on the left postero-lateral tongue). Clinicians have tried Tylenol#3 (acetaminaphen/codeine 300/30) 3x/day), prednisone 40 mg, clobetasol, nystatin. He denies lesions elsewhere. He has not had endoscopy, but denies difficulty swallowing. He has been to major U.S. medical centers without diagnosis or relief. Blood work is reported to be within normal limits. No known lesions in family members.
Histopathology
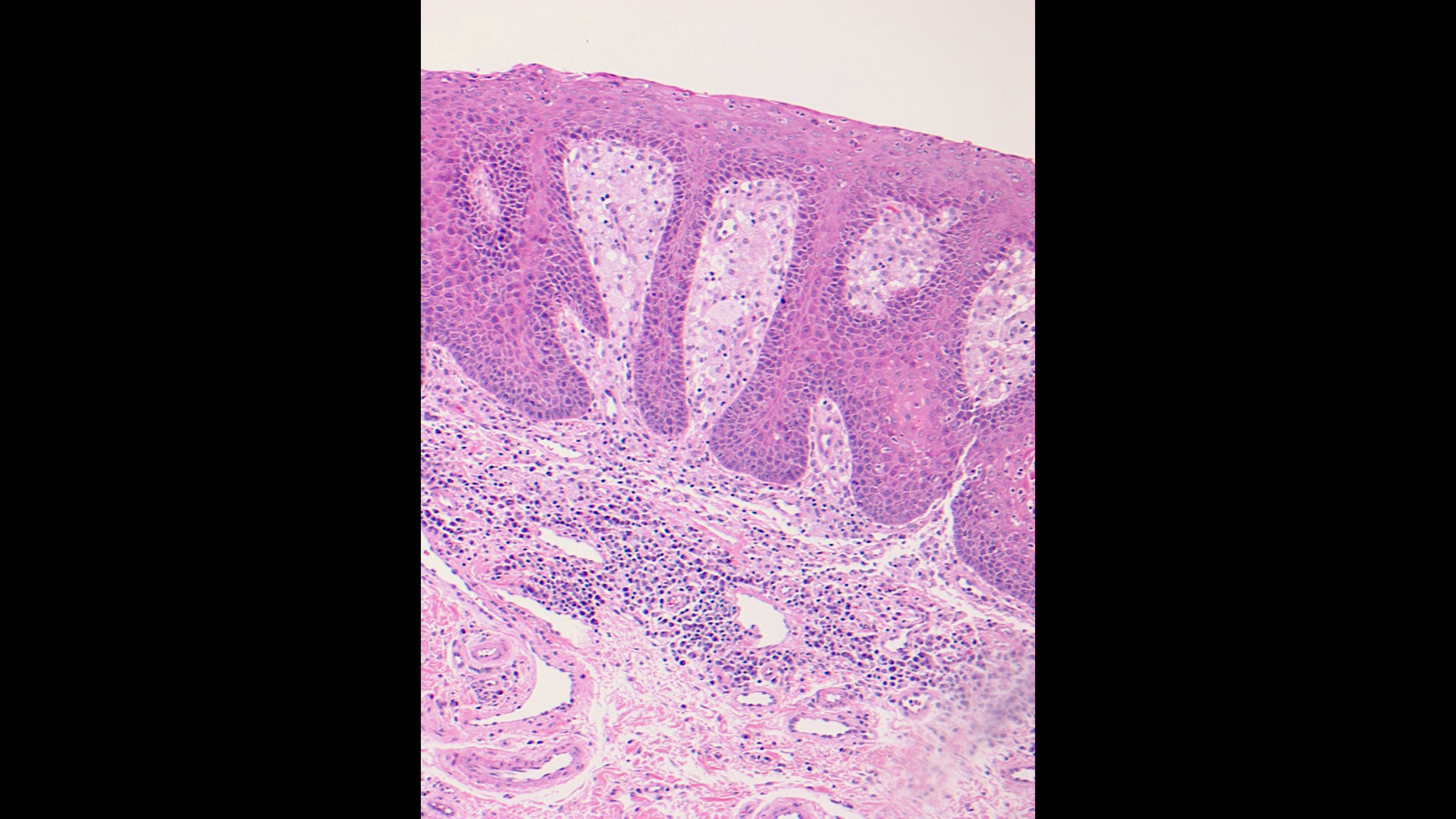
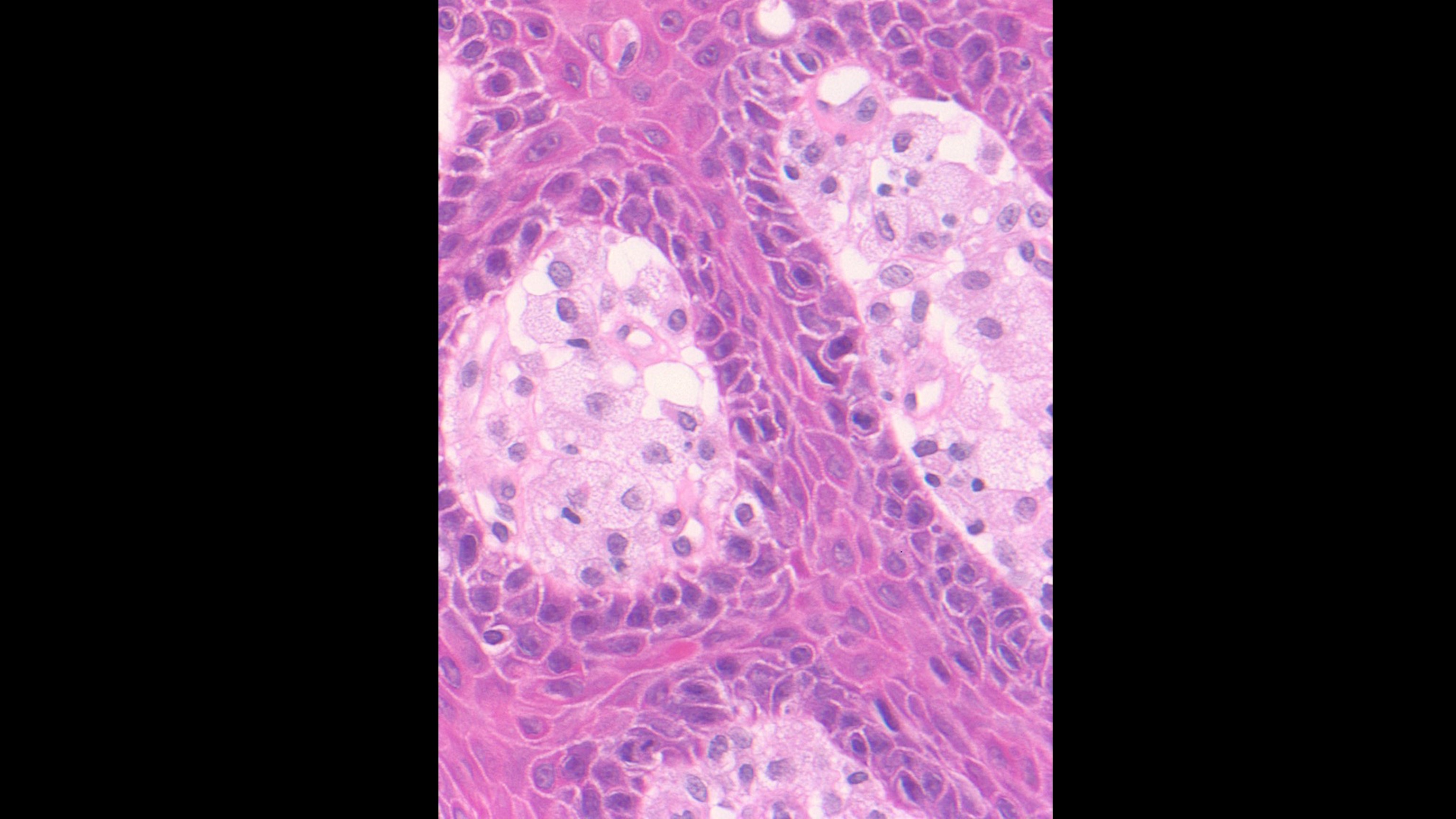
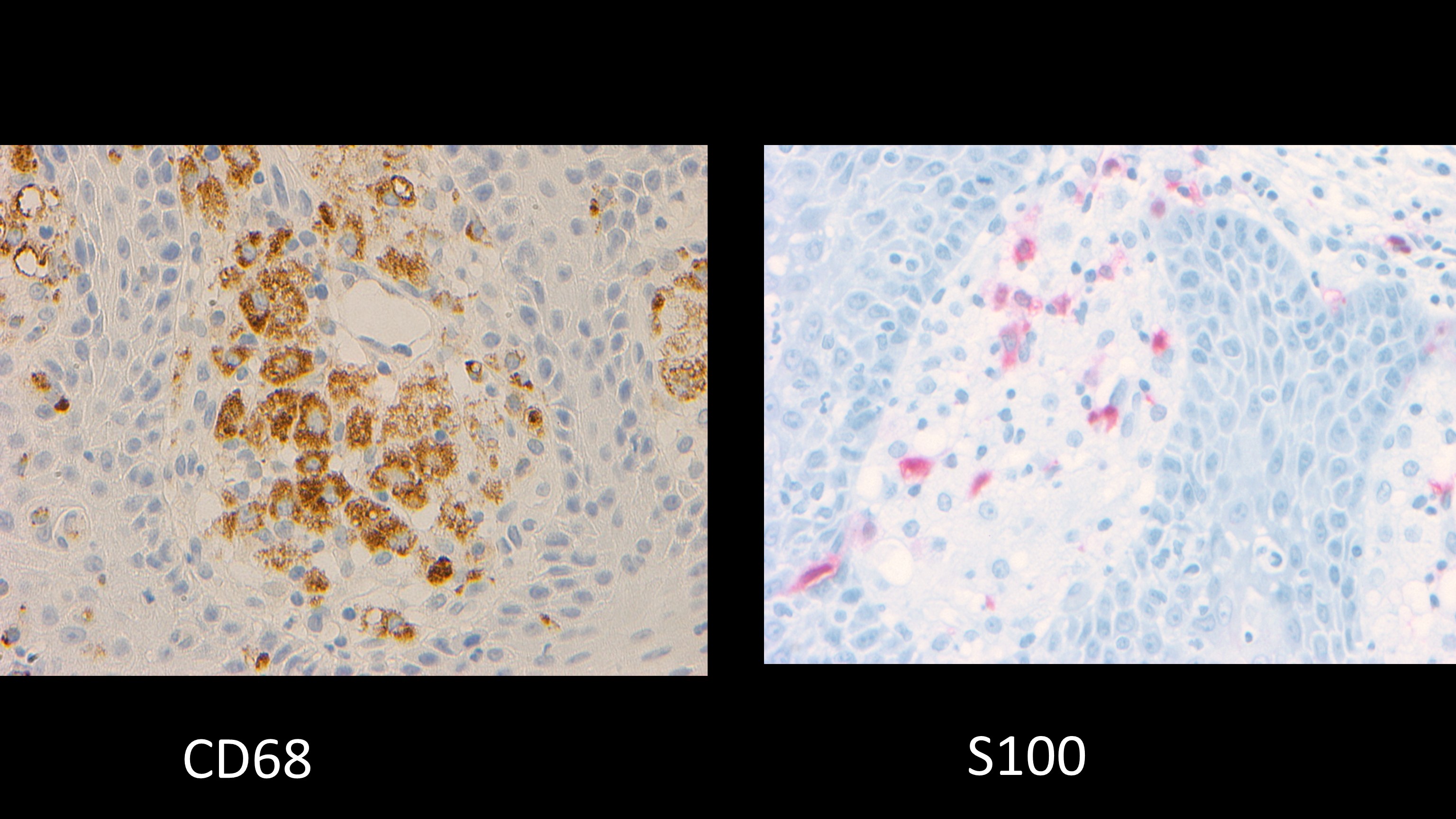
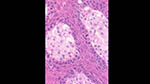
Two VX-like specimens show foamy histiocytes mostly confined to the connective tissue papilla. The specimens lack the more-verrucous surface and the orange-ish color of the keratin expected in a VX. No polarizable foreign material.
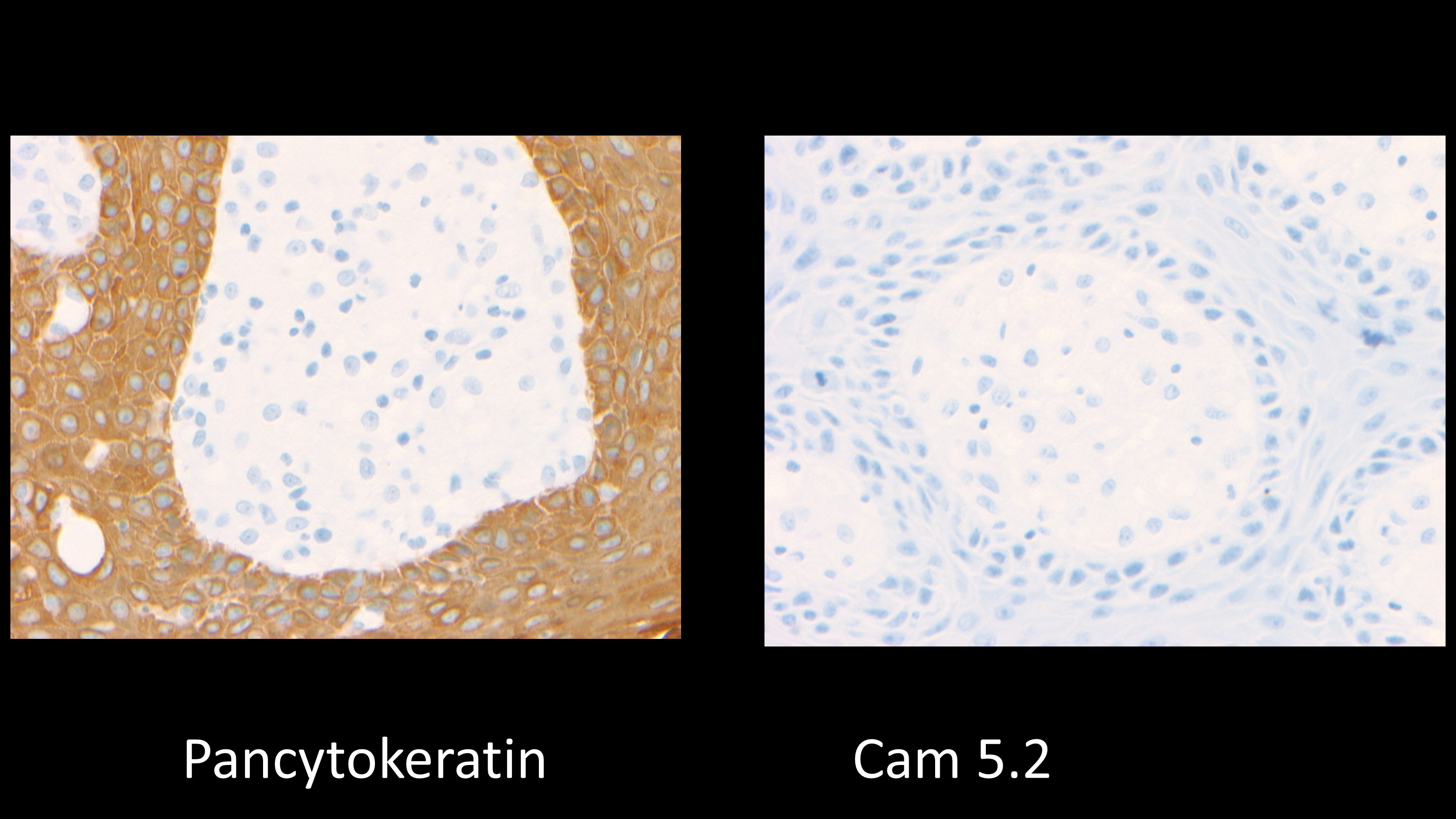
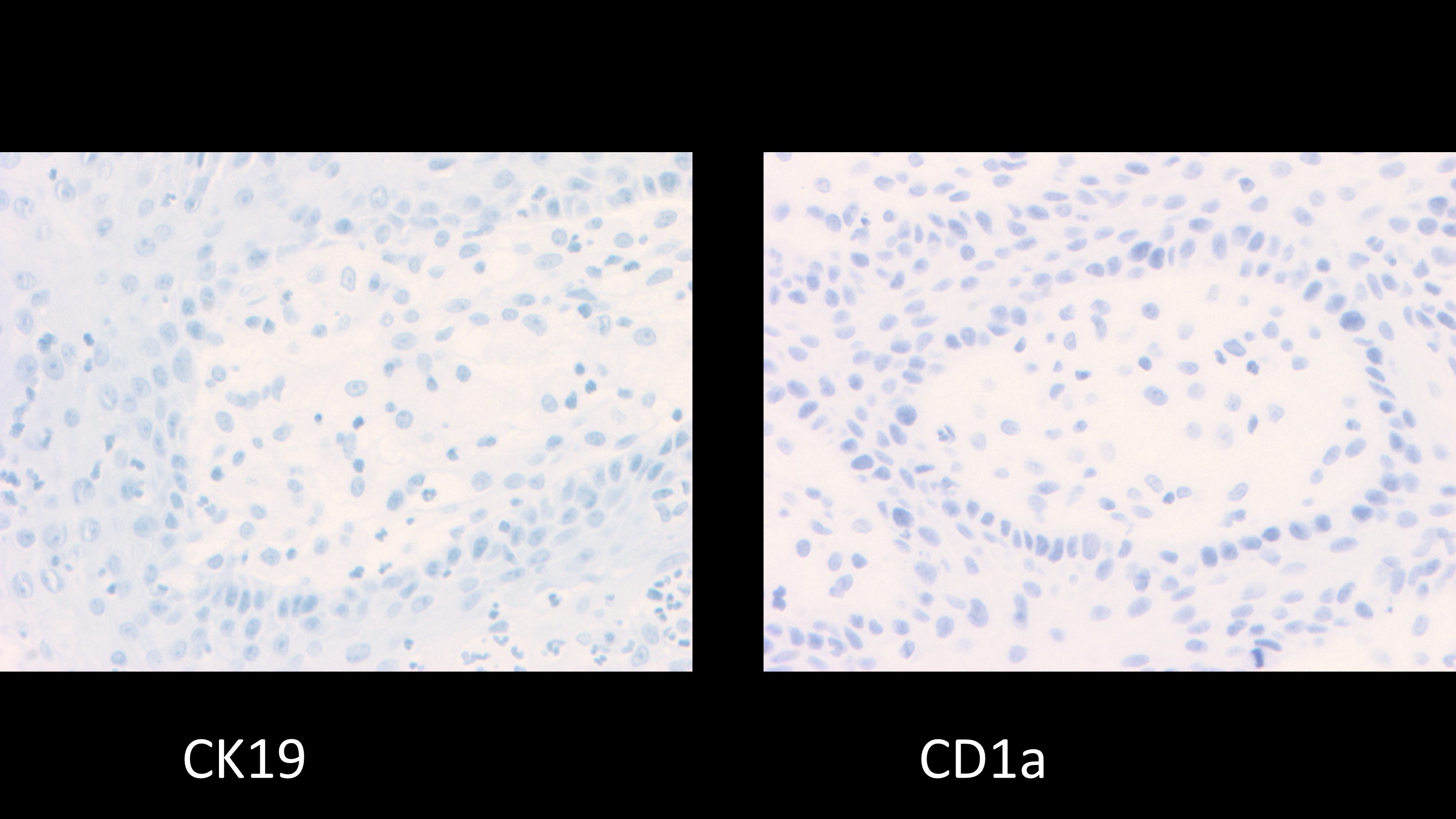
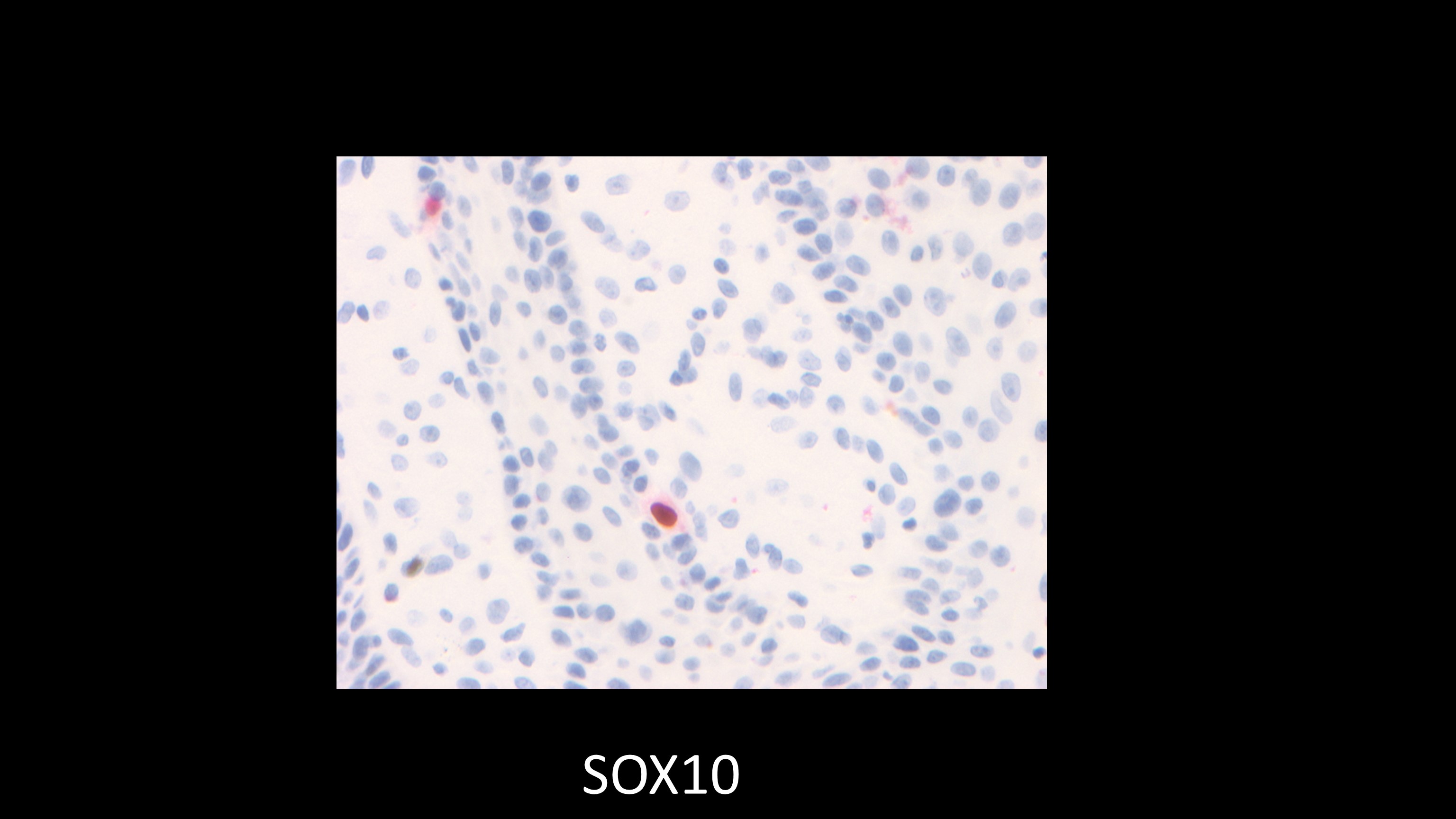
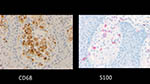
IHC: Cytokeratins negative except for an unexpected AE 1/3 positivity. Histiocytic markers positive. Could not do fat markers on FFPE tissues.
Questions
Has anyone seen a case similar to this and have a diagnosis? This does not fit the literature for multiple VX or giant VX. Any recommendations for additional IHC? (we still have several blanks), or molecular if we do a fresh biopsy? Additional specific blood work? Any cutting edge treatments to recommend? The patient is very hopeful of a resolution. Thanks to the world-wide community for your help.
Kurt Summersgill, D.D.S., Ph.D.
University of Pittsburgh
School of Dental Medicine
Images





Case prepared by Dr. Alfredo Aguirre (BBOP Manager) and Daniel Emmer (University at Buffalo School of Dental Medicine).
|