Bulletin Board of Oral Pathology
Bulletin Board of Oral Pathology
|
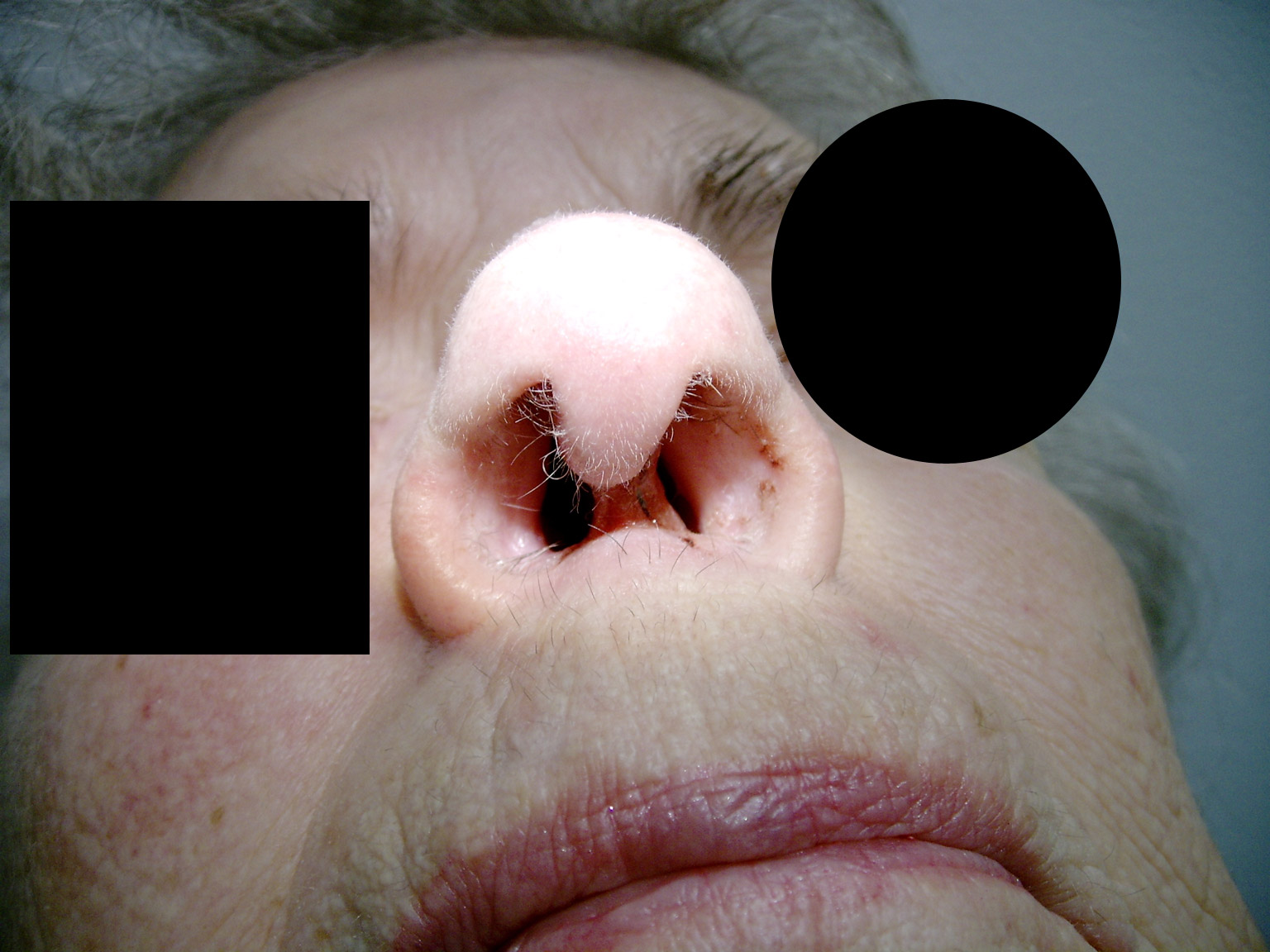
Forum for Clinical and Surgical Oral Pathology Case BBOPF 08-9 Dr. Robert Baratz (South Shore Health Care Department of Medicine, Boston University School of Medicine, Boston, MA. USA) is enlightening BBOP with a case he recently managed. This is an academic exercise and we invite your comments. This case will be on display from December 12 -17, 2008. A summary of the responses will be posted in BBOP. Then, Dr. Baratz will reveal the final diagnosis and how he managed this case. Clinical HistoryThis is an 84 year-old female, Ms. X, with a long-standing chronic connective tissue condition who has been stable on her medications for many years. She is followed by a specialist and is very compliant with her medication regimen (note: I am leaving out the name of this condition and her medications on purpose to make this exercise more interesting). Her other medical problem is hypertension which is well controlled. She has a distant history of breast cancer with unilateral mastectomy. Follow-up mammograms have all been negative. She takes lisinopril and an occasional narcotic pain reliever related to her chronic condition. She is ambulatory and mentally quite intact. Her other medications are not related to the findings in this case. Recently Ms. X was hospitalized for an orthopedic procedure and subsequently developed a DVT in her right leg. In the process of anti-coagulation it was noted she had a nosebleed and an ENT specialist was consulted. At that time a 2.0 mm small ulcer was found on her nasal septum. The ulcer began to bleed. Thus, an IVC filter was placed and she was not put on Warfarin. A few days later, in mid-September 2008 ENT biopsied the area and found chronic inflammatory cells, granulation tissue, no fungi, and no malignancy. Bacterial cultures and fungal cultures were unrevealing and treatment with mupirocin topical ointment was unsuccessful in relieving the lesion. It continued to grow in size. By mid-October 2008 the lesion had increased to several millimeters and was re-biopsied by ENT with similar results. She was now put on Cephalexin and the mupirocin was continued. Presently, November 11, 2008 she returned for follow-up and ENT reported severe erosion of the nasal septum (on both sides) and disappearance of most of the columella. Photos are attached. What is the condition and what is the diagnosis? Robert S. Baratz, MD, PhD, DDS Images(Larger images witll open in a new window or tab.)
Case prepared by Dr. Alfredo Aguirre (BBOP Manager) and Daniel Emmer (Web Administrator, University at Buffalo School of Dental Medicine). |