Bulletin Board of Oral Pathology
Bulletin Board of Oral Pathology
|
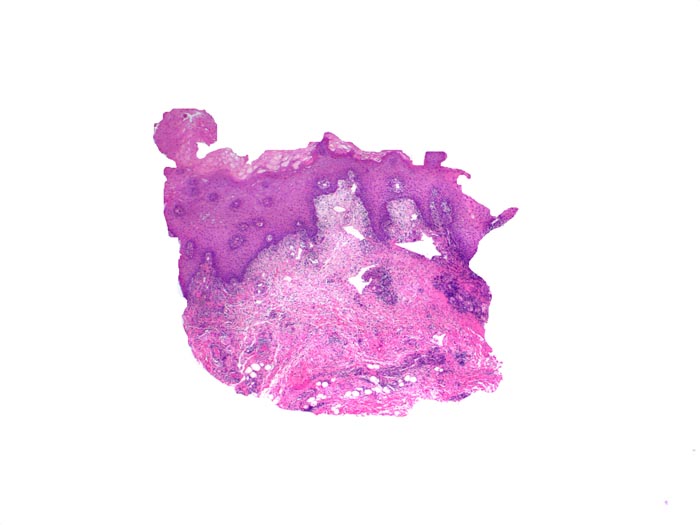
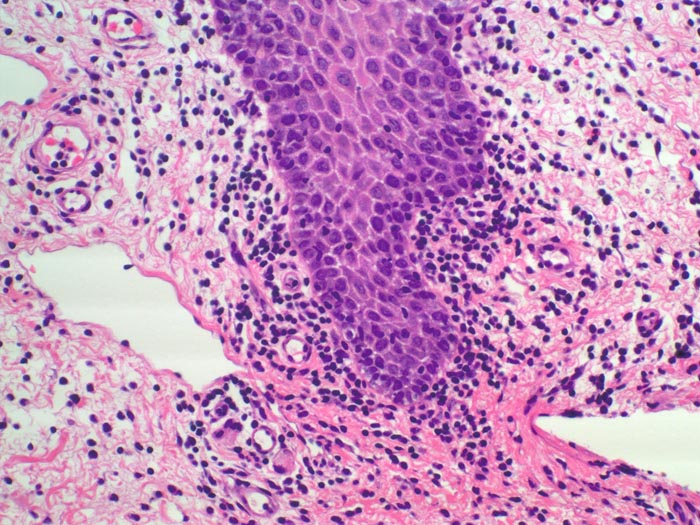
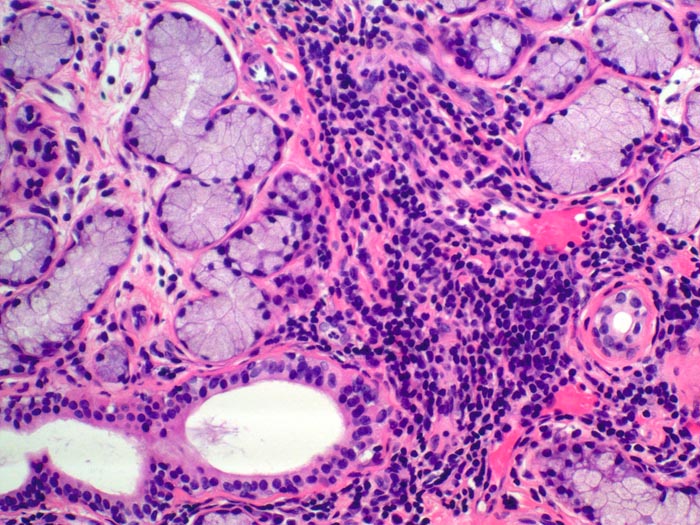
Forum for Clinical and Surgical Oral Pathology Case BBOPF 08-8 Dr. Michael Hatton and I (School of Dental Medicine, University at Buffalo, Buffalo, New York. USA) would like to invite your comments regarding a case that we are currently managing. Any suggestions that may help to arrive to a diagnosis will be much appreciated. This case will be on display from November 20 to November 27, 2008. A summary of the responses will be posted in BBOP. Follow-up of this case as it evolves will also be posted. Clinical HistoryA 14 year-old Caucasian female presented with a chief complaint of "mouth ulcers and an enlarged lip." The patient has had oral ulcers, associated with swelling over the last 8-10 months. Not seemingly associated with the foods she eats. The ulcers present with pain, and her lower lip has swollen when she is in an acute stage. The condition remits, only to have acute exacerbations. When we saw her, she was at the end of the first out of two weeks of prednisone (10 mg/day) therapy. No dental pain reported from teeth. Denies skin ulcers or sores, genitor-urinary ulceration, history of arthritis, or ocular sores. Was seen and had tests for food allergies, serum factors, and formed blood elements which were all negative and ruled out celiac disease. ROS: Patient claims recurrent erythematous, pruritic skin patches on her trunk and back in September. Physical Exam (October 1, 2008): Well nourished and well developed Caucasian female appearing stated age. No skin lesions were noted. Oral mucosal surfaces along the mandibular vestibule and lower lip positive for eryhematous macules, along with linear white, yellow striae, which had a peculiar pattern suggestive of "snail track" lesions. The erythematous patches were about 1-3mm, rust colored, and did not blanch on pressure. They were evenly distributed along the buccal mandibular mucosa and the labial mucosa surface of the lower lip. They did not extend to the attached gingiva. The remaining oral mucosal complex was within normal limits. No palpable oral or neck masses were noted. No adenopathy was present. The lower lip was diffusely swollen, without fluctuance, nodularity, or discharge from the minor salivary glands. The areas mentioned were painful to palpation. TM joints were within normal limits for range of motion and without tenderness to palpation. On October 21, 2008 a follow-up examination showed a decreased erythema of the labial mucosa. The "snail track" pattern resolved. However, there was a shallow ulcer of the right buccal mucosal-labial commissure that was tender to palpation. This was approximately 8 mm. in diameter. The differential diagnosis included oral manifestations of Crohn's disease, recurrent aphthous stomatitis and pemphigus vulgaris. Biopsies of clinically affected areas were done (left lower lip and left buccal mucosa). The H&E revealed non-specific chronic mucositis and chronic sialadenitis. The direct immunofluorescence studies ruled out pemphigus vulgaris, mucous membrane pemphigoid and erosive lichen planus. In November, she re-developed the same cutaneous pattern of erythema and pruritus. The presence of oral ulcerations, lesions suggestive of "snail track" ulcers, mucosal erythema and swelling of the lip coupled to GI tract symptoms argued in favor of Crohn's disease. However, the incisional biopsy of the lip failed to reveal the presence of noncaseating granulomas. Although we are aware that a negative biopsy does not rule out Crohn's disease, we have not substantiated such a diagnosis with laboratory tests. The patient is scheduled to undergo an exploratory colonoscopy and in addition, she will see a clinical immunologist in the near future. Any suggestions you may have to enlighten us to secure a final diagnosis will be much appreciated. Dr. Michael Hatton Images(Larger images witll open in a new window or tab.)
Case prepared by Dr. Alfredo Aguirre (BBOP Manager) and Daniel Emmer (Web Administrator, University at Buffalo School of Dental Medicine). |